Why Not an Aggressive Strategy to Covid-19?
This is a paper my brother Trace Searls wrote. Trace has a PhD in Statistics and over 20 years working in the pharmaceutical industry (Full credentials at end of his post).
I'm posting this here on his behalf to stimulate debate on how we should respond to the pandemic and whether a different approach might be better. All opinions expressed are his and not mine. 
Why Not an Aggressive Strategy to Covid-19?
Is a long-term siege strategy the most realistic approach to survive the War against Covid-19?
 We have fought this war using classical defensive approaches, however, if we continue down this path of waiting out the siege, what will be the total damage to the nation?
We have fought this war using classical defensive approaches, however, if we continue down this path of waiting out the siege, what will be the total damage to the nation?
No war is won without adapting new strategies and weapons to attack the enemy, now is the time to go on the Offensive. The empirical data has been reported that those suffering from Lupus or Covid-19 and receiving Hydroxychloroquine have not experienced dramatic issues with Covid-19 at rates seen in other populations. Four proposed offensive actions are summarized and discussed below:
1. Quickly increase the production and use of Hydroxychloroquine / Zpak (with known safety history) and other new weaponizing therapies. (Fast-track production here).
2. Continue to increase testing and availability for both the Covid-19 and anti-bodies. But testing should only be used as an assurance measure and data gathering tool, not used to determine who in the population has the anti-body and then allow to be released from isolation.
3. Release people from “Stay-at-Home” order with the new knowledge of the demographic and population densities most at-risk.
• Medical personnel receive Hydroxychloroquine as protective measure.
• Those with underlying conditions can be given the Hydroxychloroquine as a protective measure in addition to adhering to the “Stay-at-Home” recommendation
• Allow “Low-Risk” population exposure to build up anti-bodies for the future (protect the population against reoccurrence later this year)
4. Lastly, expedite the testing and manufacture of vaccines (current protocol is too slow).
Defensive Strategy
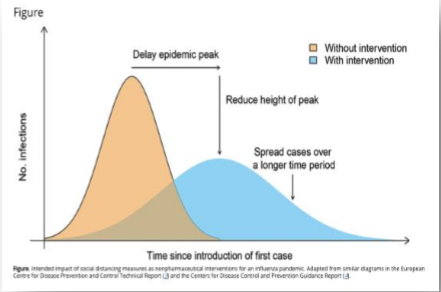
The strategy to fight this war has been largely Defensive and can be analogous to preparing for and operating under an enemy siege. The goal of this strategy has been to defensively “flatten the curve” of infection and keep the hospitalization rate manageable. With little data (sharing) and understanding of the virus (enemy) this classic strategy has always been the first action to be taken. Throughout history this strategy of isolation, limit spread and wait out the disease has been practiced.
What Do We Know (or What Has Been Communicated?)
Covid-19 is a highly contagious virus that spreads rapidly.
• Due to the speed of the spread, Hospitals can be over-run to treat those infected.
Exposure to the virus:• A vast majority of those contracting the virus will experience little to no symptoms, others will have mild to serious/conditions. The later (serious conditions) needing hospital care.
• People with compromised health conditions (Diabetic, COPD, etc.) are at high risk of serious/critical complications leading to death.
• Those suffering from Lupus taking Hydroxychloroquine have not experienced dramatic issues with Covid-19 at rates seen in other populations.
• Death Rate Models have estimated large numbers will die (hundreds of thousands to millions). But we do not know the assumptions driving the estimation, and the models now are being questioned as the expectation is not matching the empirical data.
• Due to the Government “Stay-at-Home” orders, extreme economic downturn/depression is prevalent across the country.
• Vaccine development has been communicated as promising but may not be available until Q1 of 2021 under the best projection of the protocols / clinical trials that need to be executed.
Are We Just Coping?
This defensive strategy (needed initially) now created a path of action of band-aid and coping mechanisms to confront this pandemic. It is great to see both private and government sectors coming together and embracing this effort. However, we have engaged in a large amount of energy to ration, deploy and ramp up production on PPE, ventilators, etc., to manage the pandemic in the historical classical, defense sense. In other words, are we digging in too deep to wait it out and accept a given number of casualties and economic disaster? It has even been reported that everyone should be tested for the virus and those exhibiting the anti-bodies would be allowed to be released from the “Stay-at-Home” order, (testing into compliance).
These defensive mitigation measures will flatten the curve (the models) but will extend the timetable / life cycle of the virus moving through the population. And, as many of my colleagues understand, the medical community and health agencies follow existing protocols / guidelines / regulations / norms which can be bureaucratic and slow. Moreover, we are told to worry about Covid-19 reoccurring on our population later this year, and we will not have enough of the population exposed to the virus with the development of anti-bodies to fend off the 2nd exposure.
New Weapons
Over the past several weeks, therapies have been showing promise or are being innovated to fight the virus (i.e., vaccine development, blood plasma use, exploration of anti-viral drugs). Specifically, the drug combination of Hydroxychloroquine / ZPak has been communicated as an effective therapy. However, the medical community has been hedging on the use of this drug by citing a lack of “randomized” clinical evidence generated per the usual guidelines, even though a drug shortage of this product has started taking place. Much of this behavior can be attributed by the medical community’s risk adverse desire to have overwhelming evidence of efficacy and safety before officially embracing a therapy. Yet, conforming to this practice during a pandemic war may inadvertently be dangerous to a nation overall (analysis paralysis). Especially, when you already have an approved drug with a known safety history.
Weeks ago, data was reported from observed Lupus patients using Hydroxychloroquine and from around the World / US for those who were suffering from Covid-19 who were given Hydroxychloroquine (small studies). The empirical evidence for the use of this drug (not anecdotal) was statistically significant (Statistical Technique - Clopper-Pearson approach to calculate the exact confidence interval for the Hypergeometric distribution). We have enough (what is called statistical power) to determine the effect of the drug is highly beneficial and can reduce the probability of those who are suffering from Covid-19 from progressing to a critical condition (needing a ventilator). The data strongly indicates the intervention is effective. .
Concluding Remarks
Managing this pandemic through "modeling" with a long-term siege strategy will only stretch out the timetable for the virus and economies to recover. A proactive approach based on knowledge of the virus and use of new weapons is needed. Risk aversion/avoidance is a classical defensive strategy. You win a war by taking practical, calculated (and sometimes aggressive) risks.
The proposed concepts are presented at a high level and may not be embraced by many (fear of risk taking, politics, etc.). But we should accelerate the conversation and determine the merit of each action.
Dr. Searls is a Statistician and consults with multiple industries (including Pharmaceutical / Medical Device, Telecommunications, Mining, Beverage, Legal and Government). Full bio folllows:
Information regarding treatment in other countries (compiled by Steve Searls)
Here a a few links to articles I found regarding use of Chloroquine and/or Hydroxychloroquine to treat Covid-19 patients in China, South Korea, France and limited use in New York state:
China: https://www.ncbi.nlm.nih.gov/pubmed/32074550 and https://www.jstage.jst.go.jp/article/bst/14/1/14_2020.01047/_article and https://www.nature.com/articles/s41422-020-0282-0?fbclid=IwAR2JbbZU_Hl7u...
S. Korea:
https://addictiondomain.com/chloroquine-for-coronavirus-covid-19-why-are...
France: https://www.dailywire.com/news/france-officially-sanctions-drug-after-78...
NY study: https://abcnews.go.com/Politics/clinical-trials-coronavirus-treatments-b...

Comments
Lupus Data?
Where is the data for COVID-19 in the Lupus population taking Hydroxychloroquine?
Comes from China
https://www.medrxiv.org/content/10.1101/2020.03.22.20040758v2.full.pdf
"You can't just leave those who created the problem in charge of the solution."---Tyree Scott
This isn't in a Lupus Population
This study is encouraging for the treatment of COVID-19 once you have contracted the virus but it doesn't show that taking chloroquine can prevent the disease or limit its spread. The strategy that is outlined by your brother relies on the premise that in a population pre-dosed with chloroquine, there was some level of protection. Relying on pre-dosing valuable healthcare workers with chloroquine and removing the shelter in place rules seems risky to me.
Thanks Steven
I wonder why I continue to see no mention of IV Vitamin C.
This is from early March...
https://www.worldhealth.net/news/official-statement-china-recommended-tr...
more here:
https://williambowles.info/2020/03/03/china-treating-coronavirus-covid-1...
It does appear to be in use in NYC
https://www.theorganicprepper.com/iv-vitamin-c-covid-19-nyc-hospitals/
more here:
https://nypost.com/2020/03/24/new-york-hospitals-treating-coronavirus-pa...
I suspect it isn't profitable enough to create excitement among the talking heads.
“Until justice rolls down like water and righteousness like a mighty stream.”
early treatment solves cov-19 problem, Dr Vladimir Zelenko!
https://youtu.be/-Oq6IOP1sd8
watch this!!
thanks I watched it
Informative. People should watch it.
Stop Climate Change Silence - Start the Conversation
Hot Air Website, Twitter, Facebook
more thoughts
Given that he only actually really treated only 399 people and 5 of those went to the hospital it is not actually statistically significant. 80% of the people who show symptoms never go to the hospital.
Hydroxychloroquine has side effects and at the end it was suggested that anyone receiving the treatment should get an EKG before using it because apparently there are side effects to the heart.
Still probably worth following through on.
Stop Climate Change Silence - Start the Conversation
Hot Air Website, Twitter, Facebook
The Australians are testing ivermectin to
kill the virus. If it sounds familiar to anyone that’s because it’s one of the drugs used to prevent heartworm in dogs. Don’t take your dogs’ Heartgard!
"The object of persecution is persecution. The object of torture is torture. The object of power is power. Now do you begin to understand me?" ~Orwell, "1984"
Not A Doctor, but ...
… since this is an open discussion forum, I'll go ahead and throw in my .02 anyway. It seems to me that, given the current situation, the "hunkering down," social distancing approach, whatever you want to call it, is going to have to remain in place, given the absence of an effective vaccine, until there is sufficient universal testing. Then, you can gradually release people from self-quarantine, return to work, etc., based on a couple of negative tests. Also, it seems part of the solution has got to be testing the blood for those who recovered for antibodies. To me, using plasma from recovered patients seems to make more sense as a possible treatment as opposed to betting the farm on this unproven hydroxychloroquine, or whatever it's called.
But, to me, the key has always been to develop testing materials in sufficient quantities so everyone can be tested.
What's really frustrating is to learn stuff from the MSM today about how a tiger in the Bronx Zoo was able to get tested, whereas the average person still can't get a test. And yet no one seems to point out this hypocrisy. Seems to me that the best use of the Defense Production Act is to have all the drug companies participate in producing huge quantities of the Abbott Labs product or whatever is considered the "Gold Standard" in the way of a quick test, and I wonder why those reporters in the WH news conferences aren't demanding this on behalf of the people instead of asking their BS "gotcha" questions to try and make political points.
re: testing
A flaw in your "solution" -- those that test negative twice are free to do whatever -- is the assumption that negative testees won't become infected tomorrow. Dr. Fauci, who said that he doesn't need to wear a mask because he's tested negative, made the same error. (Yet another reason why I don't accord him much respect.)
So ...
… What's your solution? Easiest thing in the world to do is criticize, but I'd prefer some positive suggestions here, I think that's what we need at the moment.
That would hurt Abbott's profits
That's why.
I've seen lots of changes. What doesn't change is people. Same old hairless apes.
I don't know about hydroxychloroquine.
The list of potential side effects is quite long, including chest discomfort, pain or tightness, and difficulty breathing. I think anyone taking it should be watched very closely.
The side effects are generally mild
but the therapeutic index is small so if you take too much you can be in serious trouble.
You're right, Steven, about Hydroxychloroquine.
These are the stats I've got. This is a global survey:
The three most commonly prescribed treatments by doctors dealing with the COVID-19 Epidemic, worldwide are:
56% analgesics,
41% Azithromycin,
33% Hydroxychloroquine
Hydroxychloroquine was overall chosen as the most effective therapy amongst COVID-19 doctors, from a list of 15 options.
The two most common treatment regimens for Hydroxychloroquine were:
(38%) 400mg twice daily on day one; 400 mg daily for five days
(26%) 400mg twice daily on day one; 200mg twice daily for four days
Prophylactic use is right on target. It is the most promising thing we could do for prevention. I read the details on how it works. It introduces genetic material into the the virus that causes it to fall apart in a unique way. Together with the Z-pac antibiotic, they teach the body's immune system how to recognize the virus and clean up the debris.
Globally, 19% of physicians prescribed or have seen Hydroxychloroquine prophylactically used to prevent infection in high risk patients, who tested negative. And 8% for low risk patients who were not yet infected.
When used to treat people who have the virus, the Drug is effective only on patients with mild to moderate symptoms. If the infection is serious and there are complications emerging or other active illnesses in the body, Hydroxychloroquine does not seem to be effective.
Doctors in the US are prescribing Hydroxychloroquine. However they are doing it wrong, according to what I read.
.
I recognize the sabotaging effect of the FDA in the above stupidity. Doctors are reluctant to use "Trump's Drug" unless the patient is going to die anyway. It could be political, or professional.
::
This drug could change the game. However in my opinion, until the US can provide masks and extensive testing for everyone — the virus cannot be contained.
Where are your stats from
The mechanisms of action you propose are not reasonable, but I am interested in the sources of the data you cite. It seems to me that prophylactic or early infection administration of hydroxychloroquine may be helpful, as you suggest.
And to add on and agree here Pluto,
This is not meant as an attack in any way,I'm not a virologist, but I am a molecular biologist (phded etc..in the late 1980's) that has used all the same methods to study life over the now greater part of my time here. And, this is unlikely to be correct:
Can you give references for this so I can see what you mean? Now you've got me genuinely curious.
Hi Steve,
I think your brother's ideas are worth entertaining, I can see, I think, how he came to some of his conclusions. I'm not a physician, but I am married to one and I have spent my research career around a lot of phd and md types who spend their days worrying about infectious diseases.
That said, I think it is worth appreciating that this is a unique situation. We've got one side that wants to *do something* (and maybe be the hero), and the other that wants to play it safe (your Offensive vs Defensive approach).
Our policy can go in various directions, and from what I've seen, the overall goal of Public Health MD/PhD sorts is to minimize death on their watch. To me, that's a reasonable goal. Alrighty then, what do you know and how confident are you feeling??
Chloroquine and all of its derivatives are *NOT* innocuous. Some people treated might well die from the treatment itself.
Your brother, as a statistician, might appreciate the twitter thread from Carl Bergstrom. He is at the UW in Seattle and is a biologist and statistics kind of guy. What he says in this thread has to do with the different modelling of Covid-19 and *why* we might not know how to go forward because different models suggest very different outcomes.
Make sure you read the whole thread if you are interested. I have to admit, I am not really qualified to critique this except to say it makes sense from everything I know. Once he goes into the rolling a ball down a ridgeline analogy and "attractors", I have to step out. I understand most of it, but I don't have the background to tell whether _truly_ it is so. Or even that it is the best interpretaion of the data. Calling Pricerip?
So read this beautiful thread (slightly biased as he is also a covid lover: see, even scientists have a hard time being completely unbiased). It compares various knowns and unknowns in two very distinctive models, worst case and best, of Covid-19 and our future.
For me, right now, we collectively don't know the best path forward.
And that's the way it is.
And that's OK.
1st do no harm is still the best way, and yes, even in a pandemic.